



ویروسهای انکولیتیک برای درمان سرطان مثانه: پیشرفتها، چالشها و چشماندازها
سرطان مثانه یکی از شایع ترین سرطان هاست. علیرغم پیشرفتهای اخیر در درمان سرطان مثانه، استراتژیهای جدید همچنان برای بهبود نتایج بیمار مورد نیاز است، بهویژه برای کسانی که نارسایی Bacille Calmette-Guerin را تجربه کردهاند و کسانی که سرطان مثانه به صورت موضعی پیشرفته یا متاستاتیک دارند. ویروسهای انکولیتیک یا بهطور طبیعی رخ میدهند یا ویروسهایی هستند که به طور هدفمند مهندسی شدهاند که توانایی آلوده کردن انتخابی و لیز سلولهای تومور را دارند و در عین حال از آسیب رساندن به سلولهای سالم جلوگیری میکنند. در پرتو این، ویروس های انکولیتیک به عنوان یک استراتژی ایمنی درمانی جدید و امیدوارکننده برای سرطان مثانه عمل می کنند. طیف گسترده ای از ویروس ها، از جمله آدنوویروس ها، ویروس هرپس سیمپلکس، کوکساکی ویروس، ویروس بیماری نیوکاسل، ویروس استوماتیت تاولی، آلفاویروس و ویروس واکسینیا، در بسیاری از مطالعات پیش بالینی و بالینی به دلیل پتانسیل آنها به عنوان عوامل انکولیتیک برای سرطان مثانه مورد مطالعه قرار گرفته اند. هدف این بررسی ارائه یک نمای کلی از پیشرفتهای ویروسهای انکولیتیک برای درمان سرطان مثانه است و چالشها و مسیرهای تحقیقاتی آینده را برجسته میکند.
متن کامل مقاله را از لینک ذیل دریافت نمایید.
Oncolytic Viruses for the Treatment of Bladder Cancer: Advances, Challenges, and Prospects

Intravesical immunotherapy with a GM-CSF armed oncolytic vesicular stomatitis virus improves outcome in bladder cancer
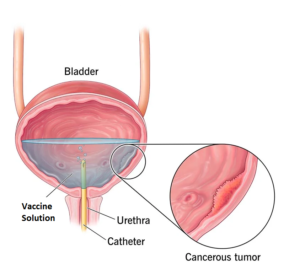
Cretostimogene grenadenorepvec is a serotype-5 oncolytic adenovirus designed to selectively replicate in cancer cells with retinoblastoma pathway alterations, previously tested as monotherapy in bacillus Calmette-Guérin (BCG)-experienced non-muscle-invasive bladder cancer. In this phase 2 study, we assessed the potential synergistic efficacy between intravesical cretostimogene and systemic pembrolizumab in patients with BCG-unresponsive non-muscle-invasive bladder cancer with carcinoma in situ (CIS). Thirty-five patients were treated with intravesical cretostimogene with systemic pembrolizumab. Induction cretostimogene was administered weekly for 6 weeks followed by three weekly maintenance infusions at months 3, 6, 9, 12 and 18 in patients maintaining complete response (CR). Patients with persistent CIS/high-grade Ta at the 3-month assessment were eligible for re-induction. Pembrolizumab was administered for up to 24 months. The primary endpoint was CR at 12 months as assessed by cystoscopy, urine cytology, cross-sectional imaging and mandatory bladder mapping biopsies. Secondary endpoints included CR at any time, duration of response, progression-free survival and safety. The CR rate in the intention-to-treat population at 12 months was 57.1% (20 out of 35, 95% confidence interval (CI) 40.7-73.5%), meeting the primary endpoint. A total of 29 out of 35 patients (82.9%, 95% CI 70.4-95.3%) derived a CR at 3 months. With a median follow-up of 26.5 months, the median duration of response has not been reached (95% CI 15.7 to not reached). The CR rate at 24 months was 51.4% (18 out of 35) (95% CI 34.9-68.0%). No patient progressed to muscle-invasive bladder cancer in this trial. Adverse events attributed to cretostimogene were low grade, self-limiting and predominantly limited to bladder-related symptoms. A total of 5 out of 35 patients (14.3%) developed grade 3 treatment-related adverse effects. There was no evidence of overlapping or synergistic toxicities. Combination intravesical cretostimogene and systemic pembrolizumab demonstrated enduring efficacy. With a toxicity profile similar to its monotherapy components, this combination may shift the benefit-to-risk ratio for patients with BCG-unresponsive CIS. ClinicalTrials.gov Identifier: NCT04387461 .
متن کامل مقاله در لینک زیر